Q Exchange
Evaluation of AQuA’s Whole System Flow Improvement Programme
- Shortlisted idea
- 2018
Meet the team: AQuA Flow


Also:
- Bernie O'Hare
- Scott Gregory
- Paul Greenwood
- Wendy Bell
- Carl O'Loughlin
Discussions with our membership led to the Advancing Quality Alliance (AQuA) identifying that poor flow across and within care systems was a major concern. Consequently in 2016, we began to explore how we could support organisations to understand flow in more detail and design an offer of support. Over 18 months the flow team at AQuA analysed and reviewed worldwide research, evidence and experience of trying to improve ‘patient flow’. Our findings are summarised in “The Challenge and Potential of Whole System Flow”, a report that was co-authored with The Health Foundation.
These ideas were developed over the 1st year including discussions at a series of workshops with AQuA members and partners. A definition of whole system flow was coproduced with members and partners and this shared definition will be the basis for future work and discussions: “The coordination of all resources across a locality to deliver effective, efficient, person-centred care in the right setting at the right time.”
Our 1st year discovery programme identified common themes, both challenges and opportunities for understanding and improving flow within care systems:
• Culture and system leadership
• Financial structures and contracting
• Capability and capacity to apply new learning and approaches
• The use and availability of information across systems
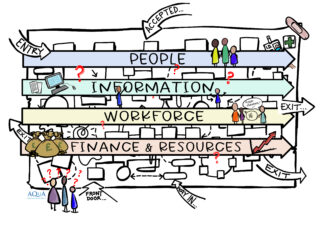
We used these themes to develop a model and supporting framework. AQuA tested this within the current NHS and Social Care context with 3 North West systems. Our model, in the image provided, shows the 4 key lines of enquiry “The 4 Arrows” that evolved over the early part of the programme as we learnt that to not intentionally explore and understand each element within a care system would prevent the generation of a shared system view of the current state.
By understanding these 4 elements of the system and their interdependencies: Risk, Leadership and Culture we were able to analyse the system comprehensively allowing us to develop the full picture before designing improvements.
We have used the Design Councils ‘Double Diamond’2 and Kreindler’s “6 Ways Not To Improve Flow” in order to develop a new model for testing within the diagnostic phase. This allowed us to remain focussed to understand the right problem we were trying to fix and not jump to solutions.
The diagnostic phase of the programme is crucial to understanding the local context and system challenges. The overarching aims for the diagnostic phase are listed below:
1. Make the system visible to itself and develop a shared purpose.
2. Create an environment for discussion and engagement across traditional professional or organisational boundaries.
3. Map the current state
4. Understand queues and waits
5. Ensure the lived experience perspective is sought and involved equally
6. Identify an optimal pathway for design and measures of success.
We identified key success measures including integrated system leadership ; understanding of organisational and system culture(s) and empowerment of staff and patients to work together on improving their care system.
The design phase of the programme has now been started with an improvement group comprising of staff different areas across the systems. This group will be using all of the information and analysis gathered during the diagnostic phase, and following the Model for Improvement to design PDSA cycles that would lead to system improvement.
These PDSA cycles will all have individual aims and a range of measures to ensure we can monitor improvement. Staff will be provided with ‘just in time’ QI and data analysis training to support this.
Simulation and modelling software will be used where possible. This software uses historic data to help test our assumptions and predict outcomes. This ensures we are implementing changes that we are confident will bring about improvement.
We are currently recruiting 5 new systems to consolidate our learning from the discovery phase and we continue to work on the design of the design phase with the original 3 systems.
We presented this work at the International Conference on Integrated Care (ICIC) on 23rd and 24th May this year and both the 4 arrows model and the impact of our approach to co-design with our Lived Experience colleagues was very well received. It would be great to have the evaluation to underpin this and bring to this conference next year.
Evaluation
The nature of this programme work means that we as improvement practitioners are very close to the teams and the work. We would appreciate and benefit from the objectivity and rigour of external evaluation on these key areas:
- Consolidation of the learning from the diagnostic phase- can we evaluate the model and the interdependencies within the phase?
- As we design the implementation phase with the 3 Discovery systems, will we see delivery of impact within the system as a direct result of our work?
- What has been the measurable impact of co-designing and delivering the programme with AQuA’s Lived Experience Panel and service users within the chosen systems?
1.
How you can contribute
- We have used Lean principles - any support from the SIG would be great.
- Any learning that can be shared about applying QI to whole systems, including the problem identification process, would be really helpful.
Further information
Diagnostic Report for Health Foundation (PDF, 1MB)
Reviewer feedback
This is a great project because…
It's good to see investment in evaluation. Improving flow across systems is key to many of the big challenges facing health and care and this should generate useful learning for the community.
By the time of the event we encourage the project team to think more about…
How to establish links with others working on flow and with the Q community - this might help inform what's going to be most useful to others and increase the chance the insight is used widely.






Comments
Wendy Lewis 28 Aug 2018
To support our Whole System Flow programme we have produced this animation - have a look! Its proving really popular when starting new work with systems with a large number of staff and community groups to reach.
https://www.youtube.com/watch?v=VaaROUdzzHY
Matthew Mezey 24 Aug 2018
Want to learn more about what Coproduction is - and isn't? Want help and advice with your own improvement project's co-production challenges?
Do join next month's zoom video call with Q's Coproduction SIG and Coproduction expert Carol Munt.
To register go here: https://q.health.org.uk/event/what-is-coproduction-and-how-can-you-make-it-work-for-your-improvement-project-with-carol-munt-zoom-call-14-sept-12-30pm/
Bring your challenges!
Deon Louw 12 Aug 2018
Hi. I would be interested in understanding the position of the emergency department in the overall flow model. In addition, when looking from the perspective of the emergency department we have 'inflow' from various sources and 'outflow' into hospital or back into the community. In relation with our own Q-project on frequent attenders to ED my feeling is that part of the problem is poor transition of care from ED to the community, and vice versa. This affects both inflow (unmet needs lead to return visits to ED), as well as outflow (engaging patients with better care structures). Our project is not flow-orientated but I can see synergies in your quote “The coordination of all resources across a locality to deliver effective, efficient, person-centred care in the right setting at the right time.”
Wendy Lewis 28 Aug 2018
Hi Deon
We spent a long time considering how much of a focus to place on EDs within our flow work! The feedback we had from AQuA membership was that they needed support to view their system(s) and community in and around the hospital in order to identify sustainable system improvements. We include ED as a component of the systems we work with and are really intentional about viewing the flows of urgent and emergency as well as planned care. The work we completed with Liverpool and are currently starting with 2 mental health organisations (looking at crisis care) will explore the reasons and impact of frequent attenders within their identified systems so I'm happy to discuss more as the work develops.
Caroline Poole 24 Jul 2018
Such a focus on improving flow, evaluating this approach for its impact will support spread and sustainability at larger scale. Important to consider flow as a 'whole system' sport - starting out with prevention and including secondary prevention.
Hein leRoux 10 Jun 2018
This is a message of support, I work for ECIP and flow is often seen as a hospital concept. Certainly hospitals have done much work on improving patient flow, but as a GP, I can see that patient flow is a system challenge both into the hospital, but also out the backdoor. Any projects that can take the flow concept out of the hospital and into the community / social care has got be to good for patient care. 'Patient time' is a great common denominator for across system working.
Lindsey Darley 21 Jul 2018
thank you Hein. We haven’t considered patient facing time as a measure yet, however this would be a good measure to triangulate with staff satisfaction with measured over time as changes are made. With the Intermediate Care Programme in Bolton we have been monitoring time away from home which includes hospital stay and would like to understand what the impact has been on longer term care needs and the hopefully reduced, impact of de-conditioning. Any more ideas gratefully received!
Thomas John Rose 25 May 2018
Hi again. The AQuA's whole flow document emphasizes the importance of process mapping. This is not the same as mapping the system flows. On page 12 of the report under the title 'Methods for understanding system flow' the report states 'The effectiveness of these approaches is often contingent on the quality of the process mapping used to inform them....' If you need any assistance with your process mapping, that is if you plan to do any, I would be happy to help. Regards Tom
Elizabeth Bradbury 24 May 2018
Evaluation of this work over the course of 2018-19 would add real value in terms of shaping AQuA's next phase of work and making the learning accessible to the wider UK since whole system flow is something we all struggle with.
AQuA will maintain links and share learning with the seven NHSI lean exemplar sites and with industry such as the Royal Academy of Engineering system design group.
Thomas John Rose 22 May 2018
Have you identified processes and mapped them?
Wendy Lewis 24 May 2018
Hello - firstly thanks for having a read of our idea!
And yes, we have mapped the system flows based on our model (people, information, workforce and finances)with our 3 discovery teams. We'll do the same with the new team we recruit but hope to do this in a shorter time frame. Our evaluation is to see of we can gather the rich info as in the discovery teams if we do the work in 4 months instead of 8.
Comments are now closed for this post.