
The Juran Trilogy has two key themes.
- Managing customer requirements.
- Managing the Service Realisation System/processes (delivery system).
Although the trilogy was first designed for manufacturing, the above two themes apply equally to the design and delivery of health care. The trick is how we implement them and retain their aims.
Let’s look at the first theme: managing customer requirements. That’s not as simple as it sounds for the NHS. We looked briefly at who your customer is in my previous blog, concluding that it is both the patient and the commissioner of the service, such as your Clinical Commissioning Group (CCG). For the purposes of managing customer requirements, it will be the body that has commissioned the service on behalf of patients.
With any services that an NHS trust offers it is not too difficult to find the set of Requirement Specifications/Standards that will fully define the requirement of that service. These include:
Then there are the service-specific Requirement Specifications/Standards. It’s important that a definitive set of Requirement Specifications/Standards are established. Your CCG, NHS England and NICE can help with this. Relevant Getting It Right First Time (GIRFT) reports will also help. The resulting set of documents must be registered within your Document Management System.
Service Realisation System – design and management
Once the customer requirement has been established and understood then the Service Realisation System/processes can be designed, or redesigned if it’s an existing service. This brings me onto the second theme: Managing the Service Realisation System/processes. Patient safety is a key consideration when designing and managing health care processes. A good indication of what is required here can be found from the following two sets of documents:
The National Patient Safety Syllabus refers to a number of schemes that are worth consideration at this point. Two of these are:
It should be noted that Safety II may complement Safety I, not replace it. The distinction between ‘care’ error and ‘delivery system’ error is also addressed in these two documents.
Patient safety is a key consideration when designing and managing health care processes.
There are two key themes throughout these two documents. These are process and variation. Both require much thought when considering designing and managing a health care realisation system.
The ISO9000 series of quality management standards recommends a process approach and I strongly back this recommendation. A process approach is well understood outside of the NHS. The QMS standards have clear descriptions and the healthcare standards, BS EN 15224 (quality) and BS EN13940 (informatics) have descriptions specific to health care.
Service design or redesign has either to fit in with current systems, such as IT systems, or new systems will need to be developed. It’s worth looking at the NHS Long Term Plan (LTP) to see what it says about IT, AI and service redesign. There is a link to the LTP in the interactive version of the illustration below.
Error and variation
Two areas that require further consideration are:
- Defining error
- How to design an allowance for a degree of variation into the design of the Service Realisation System processes.
Both are key to designing and managing a health care service. We also need to define what we mean by variation in this context and I will tackle that in a future blog.
I spoke about how a QMS can reduce error in my first blog of this series. There are two types of error in the NHS, care error and delivery system error. These are closely related to Juran’s two types of quality improvement, discussed in my second blog.
Terminology is important. For instance, error is also referred to as non-conformance, non-compliance, or adverse event. I recommend that, as far as is possible, the use of British (or ISO) standards terminology and definitions.
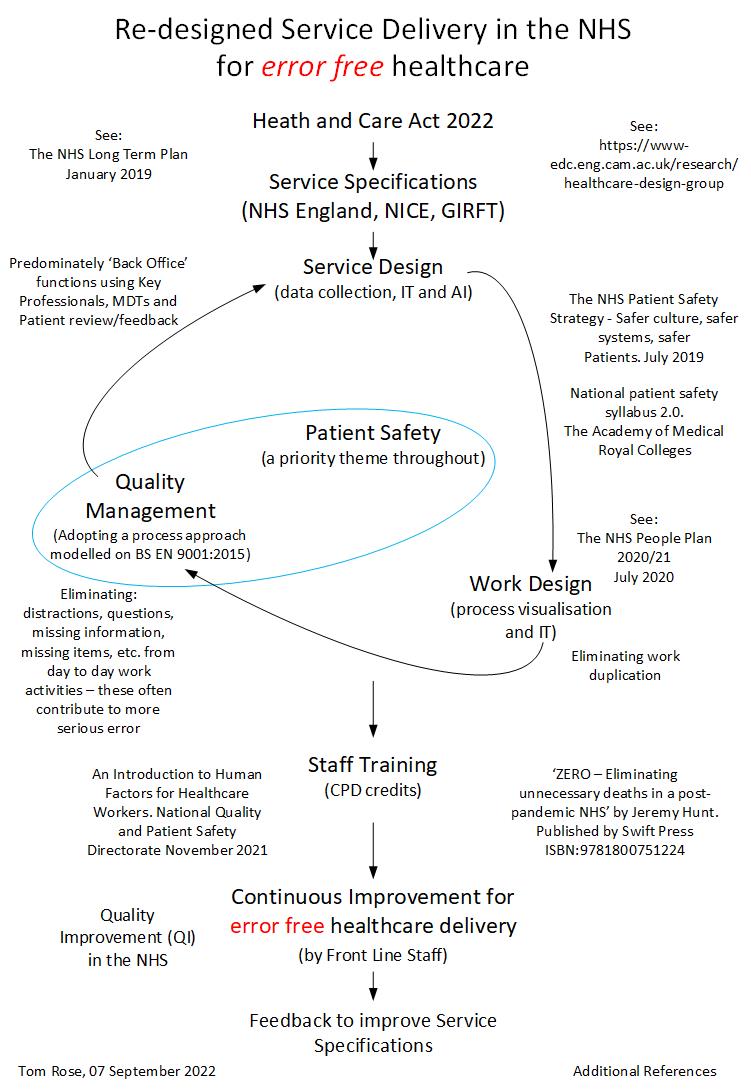
The following illustration highlights some of the issues discussed here.
Documentation and roles
You may well be asking ‘Who is going to do all this?’ That is a very good question. Service Realisation System design, Process Management System design and Quality Management System design are all extremely technical activities and require specific training and skills. It’s certainly not a job for NHS front line staff, although good documentation and training will ensure they are able to implement and improve the system once designed.
This interactive service visualisation may offer some ideas on how to document and visualise an NHS service set of processes. It’s not yet complete – the individual service processes are yet to be added. Keep your eye on the visualisation as it will be periodically updated.
To put a QMS into context, have a look at Mary Dixon-Woods’ article ‘Learning from maternity services failures at East Kent Hospitals’.
Take part in ongoing discussions on these topics and find out about upcoming events in our Quality Management in Healthcare Special Interest Group.
Resources
The measurement and monitoring of safety
Digital Health London: Delivering AI for the NHS webinar series
Comments
Helen Tucker 13 Mar 2023
Hi Tom - this is very thought provoking. I am sure there is much to learn from this approach. Thank you.
Thomas John Rose 13 Mar 2023
Thanks for you comment Helen.
Hilda Campbell MBE 13 Mar 2023
Hi Tom
Thanks for sharing, a thought provoking piece. I wonder whether engaging lived/living experience may help with some of the issues raised including engaging with front line staff around any implementation. I wonder if this publication may be of interest Catherine Durose’s book, Designing Public Policy for Co-Production: Theory, practice and change.
Thank you again for taking the time to share
Kind regards
Hilda
Thomas John Rose 13 Mar 2023
I'm sure that you are right I'm a member of the same University as Catherine and will have a read of her book. Engaging with front line staff is certainly an issue. Thanks Hilda.
Nigel Coles 14 Mar 2023
Thanks Tom, excellent article; first time I've seen the various strands put together in one piece as an entire system. Very often we concentrate on a single part of the system. This is going to require some careful thinking.
Nigel
Thomas John Rose 15 Mar 2023
I agree Nigel, for example, using the PDSA cycle at the end of the process will not solve underlying issues like poor system design.