
As Q Lab UK approaches the end of the six-month design process, our fifth workshop on 14 April was an opportunity to share and reflect on our collective learning so far. We timed the session to fall as the test teams refine and test ideas in practice to address trust and confidence in technology-enabled remote monitoring.
We wanted to share with participants four challenges and tensions that we have heard consistently in our sessions together. These are:
- Data and technology vs human interactions that add value
- Evidence we value vs evidence that ‘counts’
- Embracing discomfort: co-design and community engagement
- Equity and choice
The aim of the session was to explore our individual experiences of these before considering how to make change in the system.
Hearing from case studies using celebrity interview
We used a Liberating Structure called ‘celebrity interview’ to guide a group discussion to explore how these tensions and challenges are being experienced in different contexts, and to unlock new ideas and inspiration for navigating them.
Our three ’celebrities’ were:
- Claire Beard, Virtual Ward Manager at Norfolk and Norwich University Hospitals.
- Sadia Khan, Consultant Cardiologist at Chelsea and Westminster Hospital.
- Jill Owens, Programme Manager in the Technology Navigation team at Kent Surrey Sussex AHSN.
Claire reflected on the benefits of technology-enabled remote monitoring from a nursing perspective. The conversation then explored some of the challenges involved in convincing clinicians of these benefits when they are concerned about patient safety and clinical governance.
This served as a useful reminder to some participants about the newness of these innovations:
“It’s easy to forget that we are working on new innovative things and we don’t have all the answers… yet!” Lab contributor
Prompted by Sadia’s experience of implementing remote monitoring in the highly pressurised context of the pandemic, participants identified the value of safe spaces and taking time to reflect and learn about what is and isn’t working. Sadia shared how she acted on her concerns about access to the service. This led us to explore the third and fourth challenges around ‘embracing discomfort’, and equity and choice.
“I have had to go out and find different partnerships and different people to work with, and it’s not easy. It’s not just the time and resource none of us have. It’s about the whole new mindset […] and being really open to hear things that are sometimes really difficult to hear.” Sadia Khan
The conversation prompted powerful reflections from Lab contributors about taking ‘the courage to pause’, and to think more about what is left out of evidence and the need, not just to co-design but to ‘co-deconstruct’ and ‘co-demolish’ the systems and processes that block change.
This resonated well with Jill’s experience, which shows the importance of ‘designing for the majority by focusing attention on the minority’. Jill advocated ‘looking deeper [at] why’ people aren’t participating in the digital technology:
“[Choosing not to engage] is different to, “I have dexterity issues and I can’t use the equipment”. They are completely different things, and it’s important to drill down to who the individuals are who can’t use that innovation and why.” Jill Owens
How we tackle complex system change
After hearing personal reflections on the shared challenges and tensions, we took a step back to look at how to make change happen in a complex system. To help us with one way to think about change, we introduced Donella Meadows’ 12 Leverage Points to Intervene in a System.
This model helps to demonstrate how focusing on creating small shifts in a few things can produce big changes across a system. These focus areas are also called leverage points.
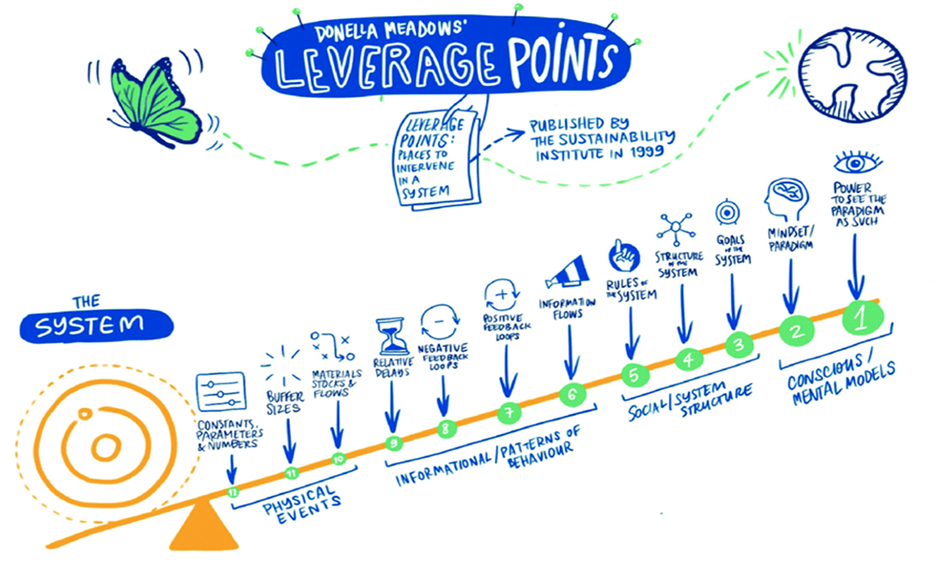
The model shows that the further along the twelve leverage points you go, the more impact you will have in transforming a system. However, the further along you go the harder things are to influence and the longer they take. This is due to the deeply rooted patterns and behaviours that influence power dynamics, relationships and mindsets.
For example, in the context of technology-enabled remote monitoring, we might try and put relationships or holistic care at the heart of the work. This could result in radically different outcomes for our system than simply increasing the volume and variations of remote monitoring products.
This model also shows that we need to be exploring the full spectrum of leverage points in our strategic planning. The Lab approach enables us to work together to identify where we are each uniquely placed to intervene in the system and find ways to coordinate our work for greater whole system outcomes.
Conclusion
The workshop brought to life some of the complexities that teams are navigating as they progress work to implement remote monitoring. It highlighted the value of exploring these issues from multiple angles; to hear the real, day-to-day challenges and concerns for clinicians; to use different types of evidence and data to “co-deconstruct” and challenge assumptions about behaviours and attitudes; and of the importance of having safe spaces to share learning and inspire others on the difficult work of change. You can read the full write up of the workshop on our website.
Let us know in the comments if these tensions and challenges resonate with you. Is there anything you disagree with or are not experiencing in your work? How are you navigating some of these issues in your service?