The case for building a Quality Management System
Fredrik Johansson joined a Q Visit to Health Improvement Scotland (HIS) to learn about their work in developing a national quality management system and how this could help deliver high-quality care.
On this page
Fredrik Johansson reflects on why organisations might want to use a QMS, key challenges of creating one, and some of the ways to approach these challenges.
The key elements of a QMS: planning, control and improvement
I joined a Q Visit to Health Improvement Scotland (HIS) to learn about their work in developing a national Quality Management system and how this could help deliver high-quality care.
During the visit, a delegate mentioned the difficulty of knowing where to focus improvement work. The conversation took me back to a recent visit to the Institute for Healthcare Improvement’s (IHI) Immersion programme which I attended as part of the Health Foundation GenerationQ Fellowship. A conversation during a workshop there came to mind.

This is exciting work but feels quite daunting. We are aware it will take years to get it right.
“How do I even know where to begin with improvement work?”
One facilitator at the IHI had posed this question to an author of The Improvement Guide, an influential text outlining the Model for Improvement (MfI), a popular approach to Quality Improvement (QI). The facilitator had started to question how far the MfI could take you when trying to deliver whole-system improvement.
The author replied: “Well, I’d assume you’d have a good quality planning process and a good quality control system so you know how you’re doing”.
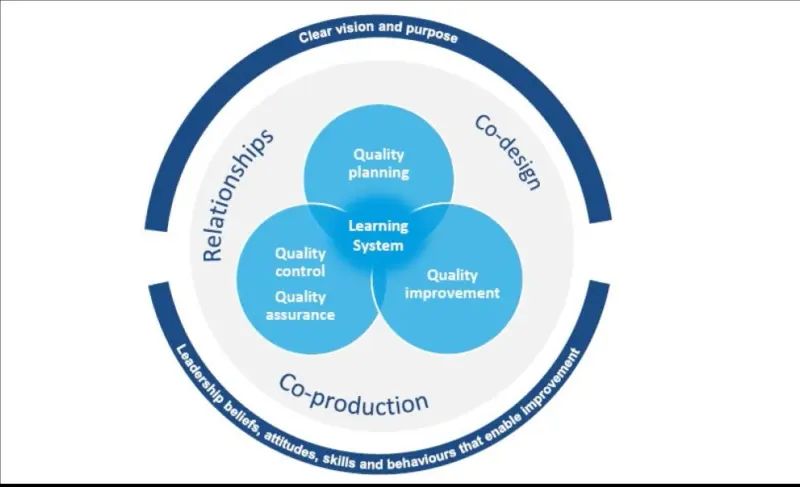
During the IHI programme and the visit to HIS we heard how QI works best as part of an improvement system consisting of three main elements:
- Quality Planning: figuring out what you want the system to deliver and how to make that happen
- Quality Control: a process of monitoring and adjusting the system to deliver the desired outcomes
- Quality Improvement: using a systematic method to improve performance and quality
Together these form what is known as a Quality Management System (QMS).
Conditions that support a QMS
During the day at HIS, sessions focused on the three aspects of QMS as well as looking at the conditions that support the system. Many interesting issues emerged; I will highlight three.
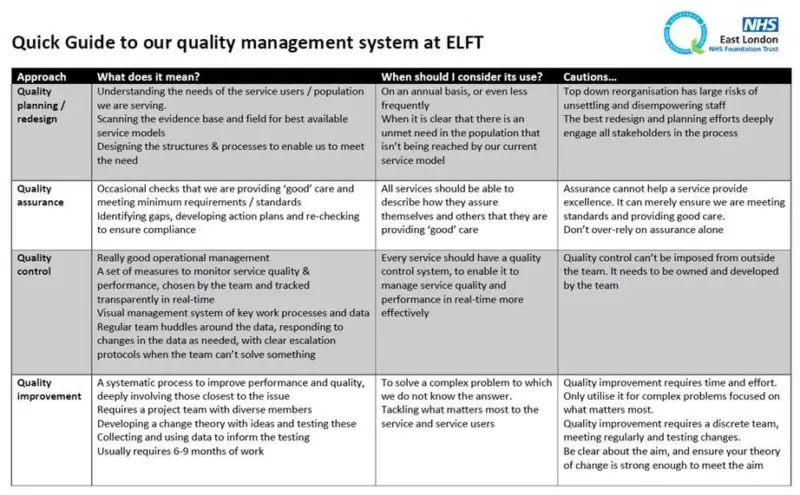
First, the role of quality assurance in health care which consists both of internal and external monitoring and inspection. Is it part of Quality Control? Ideally, assurance and control measures are closely aligned to prevent stakeholders from looking at different metrics to understand how a system is functioning. I have found that often the quality metrics that frontline clinicians, commissioners and inspectors are interested in can be quite different. Assurance processes tend to be more sporadic and quality control sits closer to the point at care delivery.
Second, HIS have outlined a set of behaviours that underpin the different phases such as focusing on collaboration and co-design and making these essential aspects of the design process in each phase. It showed me how what can be conceived as a mechanistic design process which came from industry can be used to help promote certain values and cultural norms. QMS can be as much about promoting collaboration in design and health care, an essential part of building Integrated Care Systems.
Finally, it laid bare the challenge of informatics and getting the right data, essential in developing a learning organisation. I was struck by how challenging it was to co-ordinate data on surgical morbidity and mortality from different organisations. They had worked hard at reducing the number of key metrics (from over a hundred to just a handful).
In my own early experimentation with building a small-scale QMS, I identified these key steps:
- agreeing the set of measures that can help guide teams
- ensuring this aligns with other stakeholders
- ensuring the data quality is good and then making it accessible
- making it feel like it is owned by teams at the point of care – this is a real challenge.
Like many trusts in the UK, my organisation has developed a QI team over the past few years. Many of our staff have trained in QI methodology, and lots of projects are happening. There has been real excitement from leadership about the potential of QI in providing better care in challenging circumstances. Quality improvement, Don Berwick points out in Curing Healthcare, is where most places start.
HIS have outlined a set of behaviours that underpin the different phases such as focusing on collaboration and co-design and making these essential aspects of the design process in each phase.
While I have seen great work and clear improvement by a team (or ‘micro-system’) it is harder to feel confident about the impact across the whole system and on whole-system outcomes. This step, from micro-system to whole-system improvement feels huge.
HIS have outlined a set of behaviours that underpin the different phases such as focusing on collaboration and co-design and making these essential aspects of the design process in each phase.
The Health Foundation publication The Improvement Journey provides a great overview of this challenge and thoughts about how to make the leap. It highlights the importance of aligning activity across the system and that teams focusing on their pet improvement project can detract from the system as a whole improving.
I think this is what Gary Kaplan (Virginia Mason CEO) was talking about at a recent International Forum when he said the QI projects could be damaging to an organisation. That is, energy and enthusiasm being spent locally without attention to whole-system problems, and spread and scale-up of improvement work.
In essence, this feels like what a QMS in health care is about – purposeful design of each part of the system, understanding how each micro-system can help achieve common goals, creating shared purpose where improvement activity can be co-ordinated and amplified.
Our Trust Board recently approved our proposal to start development of a QMS. We are developing some prototypes with individual teams, and are working together with our informatics team, performance committees and Quality Governance so that we can build the data system and be clear about all the competing demands of the teams involved. We have also begun mapping out how we can create a Board-to-Floor golden thread that helps each part of the system understand how they contribute to a shared outcome.
A strategic and operational approach to QI planning
This is requiring our QI team to work more closely with many other parts of the system, to understand the demands and expectations of each part of the system. At the same time we are trying to allow the teams themselves a strong voice in building their own QMS with metrics that matter to them and their service users.
We have also been trying to develop a stronger QI presence at senior strategic and operational levels to support Quality Planning work, drawing in frontline teams into this work and agreeing together on what the system is hoping to achieve, and how we can deliver this. Historically there has been a disconnect between planning at senior level, where Key Performance Indicators are negotiated with commissioners, excluding the teams delivering the services who should be overseeing quality control but who are disinvested by not being involved in the process.
This is exciting work but feels quite daunting. We are aware it will take years to get it right. But if we do I think we will be closer to realising the potential that QI has beyond the team-level to improving the whole system.