Q Exchange
Peer support in mental health crisis care
- Idea
- 2018
Meet the team: Peer ASSiST Sheffield

Also:
- Sue Sibbald – Peer Expert SHSC FT
- Danielle Chadderton- Peer Recovery Worker SHSC FT
- Linda Wilkinson- Director of Psychological Services SHSC FT
- Alex Pavlovic- Consultant Psychiatrist in Medical Psychotherapy SHSC FT
- Sheffield Health and Social Care Foundation Trust
The Challenge
We know that suicidal behaviours are very common in people with emotional sensitivity who may be
labelled with ‘ Personality Disorder’. Research has shown that between 8-10% of
people with this difficulty will complete suicide, more than 50 times the general population rate of suicide (Linehan
2006).
People who experience complex trauma and emotional sensitivity (Personality Disorder)
can often find themselves in crisis, with recurring suicidal behaviour and self harm.
For some people this can sit alongside transient psychotic experiences, as well as intense
anxiety, depression and anger. As a result some people can be regular users of psychiatric and acute hospital
emergency services.
From crowd sourcing on Twitter somebody describes what it felt like to be in a mental health crisis.
“Being in so much turmoil that all my thoughts are about ending it, and now not later. So
fed up that things are never going to change. The need to escape is great.
Anywhere off this earth will be better.”
However, once admitted to the ward impulsive and high risk behaviour can escalate, causing concern for the service user and staff. This can often lead to longer lengths of stay on the ward and restrictive interventions.
We want to work with peer experts to offer an improved service user experience of mental health crisis care.
The Idea
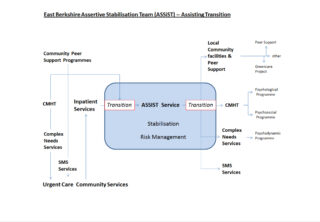
We are looking for funding to employ peer workers to work alongside clinical staff as an Assertive Intervention Stabilization Team (ASSiST), offering a 12 week structured psychosocial intervention for people with complex trauma and/or emotional sensitivity who are in crisis on acute wards or with the Crisis/Home Treatment teams. The ASSiST model was developed by Dr Rex Haigh and Dr Natasha Berthollier in Berkshire. The overall aim of the model is to offer an in reach to service users who are in crisis, focussing on increasing resilience through the development of strategies to manage emotional problems and risk behaviour in a community based setting,
thereby reducing the use of Mental Health inpatient services when safe, effective alternative is available. Peer workers can represent hope and explore treatment options in an atmosphere of optimism and empowerment.
The ASSiST Model has been comprehensively evaluated and has been shown to be successful:
- Improved service user experience of care
- Reduced length of stay on acute wards and with Home treatment teams, leading to reduced costs which have been re-invested in community services
- Improved outcomes for Service users
The Plan
Over the last 6 years SHSC FT has been working on improving the quality of care offered to people who experience mental health difficulties associated with complex trauma and emotional sensitivity.
Following a review of services, we employed a Peer Expert to coproduce and deliver a staff-training package and psycho education groups for service users, family and friends. We now employ a number of paid
peer recovery workers and the plan would be for the peer workers on the ASSiST programme
to be supported by this existing network.
Staff in SHSC FT have already visited and established good relationships with Berkshire and the next steps are for Dr Haigh and Dr Berthollier to run a workshop for staff and service users in Sheffield.
We will collect pre and post outcome measures, including bed usage, to compare with Berkshire and to put together a business case to reinvest savings to create permanent peer recovery posts.
Existing links
- the Berkshire ASSiST team
In Sheffield:
- Rethink who provide the SHSC crisis house
- local Emergency departments and Liaison Psychiatry
- the University of Sheffield (for help with outcome measures and research)
Who benefits
- Service users – they tell us that input from peer workers helps them helps them to hold hope, to feel empowered and more connected
- Peer recovery workers report feeling that employment gives independence and a sense of purpose and a sense of empowerment about improving services
- Staff working in the Trust
- Q Community: we will share this model and our broader experiences of working with peer experts within SHSC FT and offer opportunities for Q members to visit. Our Peer Expert Sue Sibbald has a national profile around service developments for people with emotional sensitivity. We will work to give regular updates on the developments and use social media, blogs, Twitter and other established platforms to reach out to generate broader interest and reach out to harder to reach service users.
We recognise that the Sheffield care pathway for complex trauma/emotional sensitivity needs to evolve further and we want to continue to improve, with co-production at the heart of new developments.
We are also keen to contribute to a body of practice-based evidence to support service users to receive improved quality of care, and ultimately to reduce self-harm and completed suicide.
How you can contribute
- Experience of what works when you are trying to implement successful ideas from another area
- Any ideas about how we can make this work in Sheffield




Comments
Helen Crimlisk 14 Jun 2018
Just heard some more detail about the background to this project. I’m interested to understumore about how you plan to support these workers. Do they need bespoke supervision or is this provided within the team in which they are embedded? Or both? And if so how do we ensure it is not over burdensome?
Harriet Fletcher 20 Jun 2018
Thanks Helen for your other comments - and this is a really good point. As you've highlighted the CMHTs have had peer support workers for a couple of years and there is an established structure in place already: the plan would be that they would be offered line management support by the clinical psychologist in the CMHT Recovery teams, and supervision from an experienced OT who has a background in employment support (with back up from clinical psychology staff).
The peer staff would also join the peer network monthly meeting monthly, which offers support and opportunities for CPD.
Sue Sibbald (our Peer Expert, part of the bid team) accessed an introduction pack for peer workers from Scotland which has been very useful in supporting the delivery of a good induction to working in mental health services.
Hawys Tomos 11 Jun 2018
Wonderful to see a peer support bid. I see that Dani is part of your team so you’re hopefully already aware of the work the Q Lab has been doing around peer support. Perhaps you could utilise the ‘peer support hub’ that’s being developed by National Voices to disseminate your learning too, when it’s up and running.
Harriet Fletcher 20 Jun 2018
Thank you! - yes, Dani and also Lee Lester have been really helpful in sharing their learning from the Q Lab work they are involved with. I think using the Hub to disseminate the work will be really important.
Ruth Wilson 8 Jun 2018
Great idea, providing support and improving quality of care for people by people who have lived experience of mental health conditions.
Jo Hemmingfield 1 Jun 2018
What a great idea for a project! I like that the peer workers will be part of a team that has co-production at its heart.
Helen Crimlisk 19 Jun 2018
SHSC has had peer workers for a couple of years now, embedded into CMHTs. I has had a real impact not only on patient experience and care, but also on something a little less tangible - compassion, culture, the recognition that it is not "them and us" which can lead to burnout and poor care.
Helen Crimlisk 21 May 2018
Love this, personality disorder is a really important area to address where peer working has a good evidence base not only to improve patient care but also to help staff understand this stigmatised issue.
Helen Crimlisk 21 May 2018
This looks really good, building on your successful Peer Working in CMHTs – Good luck
Comments are now closed for this post.