Q Exchange
System Wide Human Factors Learning following Mental Health Serious Incidents
- Idea
- 2018
Meet the team: # NTW Lessons Learnt


Also:
- Lorna Smith, public health registrar
Aims / who will benefit:
We aim to foster engagement with our multi-agency partners and a learning rather than blaming culture by promoting an understanding of human (systems) factors that contribute to serious incidents in order to learn lessons across the wider health economy and improve our care/contact for those with mental health problems. Learning lessons after serious incidents aims to reduce potentially preventable deaths. Multi-agency partners will benefit from peer support and we will engage bereaved families in learning events, in keeping with national guidance.
The case for system wide learning following serious incidents:
Integrated care systems are emerging and partnership working between health, social care, commissioners, primary care, third sector and others is accepted as necessary to develop sustainable care models. A challenge facing complex systems is how we share lessons learnt from serious incidents outside individual organisations. This is especially true for mental health related deaths where individuals may have been in contact with multiple agencies prior to death. Guidance on Learning from Deaths (National Quality Board, 2017) revealed that organisations investigate and learn from incidents to varying degrees and there is no standardised investigation methodology. Human or Systems Factors methodology however has been used widely in the aviation, rail and nuclear industries and came into prominence in health more recently. It is therefore a cross-cutting, evidence based method of investigating serious incidents across multiple agencies. Unless robust patient safety science methodologies such as Human Factors are used to investigate and learn from incidents, we are at risk of focussing myopically on what appear to be individuals’ errors rather than taking a whole systems view of contributory factors. This not only perpetuates a culture of blame but also means there is a lost opportunity to improve systems and processes in a place- based system of care and to introduce barriers that could design out errors and reduce the number of potentially preventable mental health related deaths.
Northumberland Tyne and Wear (NTW) Trust Serious Incident process:
Over the past two years, we have embedded Human Factors analysis into our serious incident process in line with the recommendations from:
2013 National Quality Board Concordat
2015 NHS England Serious Incident Framework
2016 Health Education England Learning to Be Safer Programme
2016 CQC report- Learning Candour and Accountability
2017 National Quality Board Guidance on Learning from Deaths.
An internal audit of our serious incident process indicates we have improved the quality of investigations in several domains, including training of investigating officers in Human Factors, staff (second victim) support and incorporating bereaved families’ concerns/questions into the terms of reference for investigations. Our action plans are more focussed on systems improvements rather than staff training/supervision or the need to generate new policies, meaning action plans are more in keeping with the Hierarchy of Interventions Effectiveness than they were prior to our introduction of Human Factors.
The How:
Taking the lead as a mental health trust in raising awareness of Human Factors in incident analysis aims to help standardise and improve the quality of investigations for mental health related deaths involving multiple agencies and enable transparency about system weaknesses in an integrated care system. We plan to:
-Host 2 half day workshops to map our investigation processes, understand how we learn lessons within individual organisations and how we could share lessons across organisational boundaries
-Thereafter NTW clinical lead for quality and safety proposes hosting a bi-annual forum for sharing lessons learnt from complex mental health related serious incidents that have involved multiple agencies utilising simulation methods to afford practical experience of Human Factors models, vignettes and teaching from subject experts on topics of interest which will aim to cover both mental health and physical healthcare of those with mental health problems.
-Engaging and learning from bereaved families will be crucial to these lessons learnt events. We will aim to develop the bi-annual learning forums with a model of co-production in mind.
-Project management support will focus on policy initiatives, process mapping, data collection, quality science methodologies, governance issues as well as evaluation and sustainability of the project which will aim to preserve a lessons learnt “memory”.
Pre-existing resources:
NTW has a clinical lead for quality and safety and a simulation lead, both of whom can deliver learning lessons events with simulation aids. We also have an ambulance mental health lead, a nurse police liaison lead and a primary care mental health lead. We attend local commissioners’ serious incident panels. We have links with the northeast public health mental health lead.
Evaluation:
-Process mapping of individual organisations’ investigation processes
-Action plans- are they proximal (related to individuals’ errors) or more systemic? Are they S.M.A.R.T?
-Thematic analysis of action plans
-Baseline safety culture tool
-Qualitative feedback- do staff feel blamed after an incident? How is learning shared? Are families engaged in incident analysis?
How you can contribute
- -Further suggestions for evaluation
- -How IT support can support the initiative
- -Potential barriers
- -
Further information
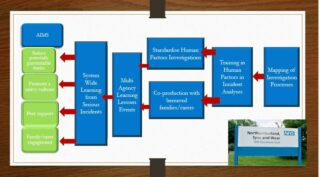
BID HF Driver Diagram (PPTX, 1MB)



Comments
Steve Yarnold 4 Jun 2018
Human factors, multi-agency working and improving Mental Health Care... We seem to have similar goals with different strategies. Shame we're at other ends of the country because we might have been able to collaborate. We are looking to develop a simulation training syllabus with a focus on multi-discipline and multi-agency scenarios to improve the physical health outcomes of people with serious mental illness. Please look up or proposal #SimInPsych and let me know your thoughts. Very best of luck!
Garry Schulz 23 May 2018
Looking forward to meeting up with you both to hear more about this. It sounds like a particularly powerful way of learning. I particularly like the focus on working across organisations, the objectivity of seeking to improve the system (instead of looking for someone to blame) and the comfort bereaved families will certainly feel from knowing that we're striving to prevent serious incidents being repeated (and encouraging them to be part of that learning and improvement cycle).
Comments are now closed for this post.